67 male with scrotal swelling
This is an online E logbook to discuss our patient’s de-identified health data shared after taking his/her/guardian’s signed informed consent. Here we discuss our individual patient’s problems through a series of inputs from the available global online community of experts intending to solve those patients' clinical problems with collective current best evidence-based inputs
PRESENTING COMPLAINTS:
Left Scrotal swelling since 1 month.
Right scrotal swelling since 2 weeks.
Pain in Left scrotum since 4 days.
Fever since 4 days.
Decreased food intake since 4 days.
Vomiting since 3 days.
Decreased urine output since night.
HOPI:
A 67 year male presented with left scrotal swelling since a month, slowly progressive initially; associated with pain in Left scrotum ß 4 days. History of Right scrotal swelling since 2 weeks, slowly progressive not associated with pain. History of high grade Intermittent fever associated with chills relieved spontaneously followed by sweating since 4 days; History of decreased food intake since 4 days because of nausea. Vomiting since 3 days non projectile, bilious (3 episodes daily). History of decreased urine output since night. Patient sought for consultation and now admitted for further evaluation and management.
PAST ILLNESS:
No comorbidities.
PERSONAL HISTORY:
Appetite normal.
Food intake decreased.
Sleep decreased
Non vegetarian
Smoker, daily 18 beedi since 30 years.
Alcoholic, 90 - 200 ml daily since 30 years.
GENERAL EXAMINATION:
Patient was conscious and coherent.
HR : 92bpm; RR: 22cpm; PR: non recordable; SBP : 50 mmHg, DBP: non recordable; GRBS: 217mg/dl.
CVS: S1,S2+, no added sounds;
R/S: BAE+, Diffuse wheeze;
P/A : Soft, Non tender, BS+, B/L scrotal swelling, scratch marks with skin exfoliation over the left scrotum.
CNS: NFND.
EXAMINATION OF INGUINO SCROTAL REGION:
B/L Scrotal swelling.
Tenderness of left scrotum.
Tenderness over the left inguinal region.
Exfoliation of skin with irregular borders present over the left scrotal region.
No swelling of penus.
COURSE IN THE HOSPITAL:
A 67 year male presented with the above mentioned complaints, Upon arrival to casuality he was conscious and coherent, initial evaluation was done and peripheral pulses absent, peripheries are cool, diastolic BP was non recordable and SBP was 50 mmHg; he was in severe scrotal pain. Fluid resuscitation was done immediately after taking an ABG and IV Analgesic, Antacid and Anti emetic were given. IV NORAD infusion was started @5ml/hr.
ECG at presentation:

ABG showed metabolic acidosis, he was started on bicarbonate correction. Mean while routine investigations were sent. USG abdomen with inguino scrotal region was done which showed E/O:
1. Rt testis: 40×38mm, Left testis: 38×20mm in size with both testis of normal echotexture and normal vascularity.
2. B/L spermatic cord and epidydimis appears inflamed.
3. Moderate free fluid with internal echos are noted in left scrotal sac.
4. Free fluid noted in left scrotal sac.
5. Spleen 8.5cms.
6. Right kidney 9.5×4.2 cms, Left kidney 9.8×3.6 cms, both kidneys are of normal echotexture, Corticomedullary differentiation present and pelvic calyx system is normal.
7. IVC 20mm.
Impression of B/L Inginoscrotal USG:
1. B/L Epididymo-funiculitis (L>R).
2. B/L Hydrocele (L>R).
3. Diffuse scrotal wall edema.
FEVER CHART:

Investigations Chart:

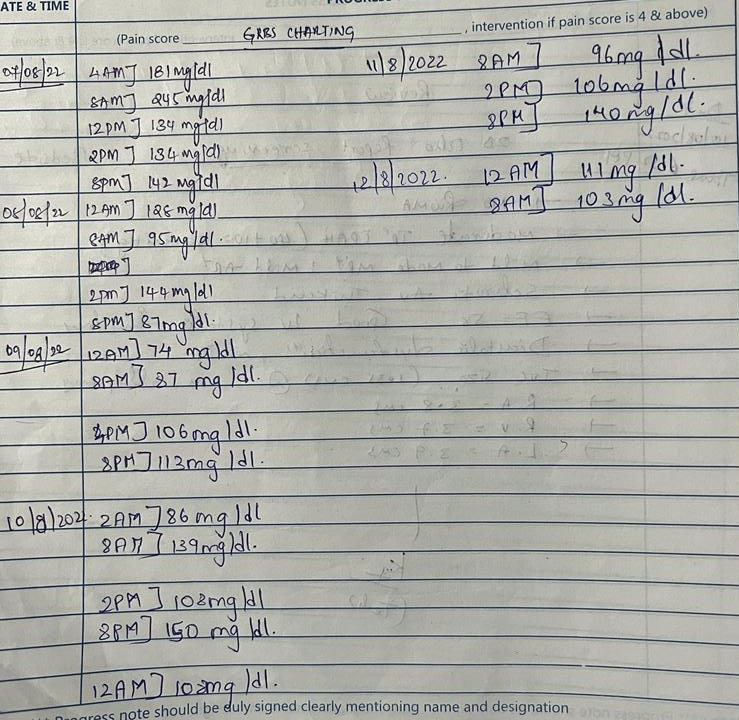
GRBS TRENDS:
Chest XRay PA



His BP was 80/60 on NORAD infusion @4ml/hr.
2d ECHO was done on 07/08/2022, which showed:
No RWMA, Moderate TR with PAH (55mmHg), Mild MR, Trivial AR, Sclerotic and thickened AV, EF 58%, Good LV Systolic function, Diastolic dysfunction, No Pericardial effusion, IVC 1.75 cms which was dilated and non collapsing, RA and RV dilated, Mild dilation of LA.
Scrotal examination on day 0 admission in the evening:
Increase in scrotal swelling extending to the penus, tenderness of the left scrotal region, left inguinal region and penus. Excoriation of the left scrotal region remains same.

On day 1, surgical review for the swelling has been done and scrotal support was placed, to reduce the scrotal and penile edema. De-escalation of Inj. NORAD was done. His BP was maintaining at 110/70mmHg. He was having intermittent high grade fever. His scrotal pain has been reduced and slight decrease in swelling of the scrotum. There are appearance of blisters over his penus. As there was soakage of scrotal support, dressing was done and a new scrotal support was placed.



Clinical Images of patient:
DAY 0:





TREATMENT:
1. IVF NS/RL @ 100ml/hr.
2. INJ. PIPTAZ 2.25 GRAMS/ IV / STAT.
3. INJ. LASIX 20 MG / IV / BD.
4. INJ. PAN 40 MG / IV / OD.
5. INJ. ZOFER 4 MG / IV / SOS.
6. TAB. DOLO 650MG/ PO / SOS.
7. VITAL MONITORING & TEMP CHARTING.


Comments
Post a Comment